




Endophthalmitis can be categorized based on the etiology of infection: acute-onset or delayed-onset postoperative, conjunctival filtering bleb/tube–associated, posttraumatic, endogenous, intravitreal injection–associated, and keratitis-associated. The prophylaxis, diagnosis, and treatment of endophthalmitis has evolved over the decades.
Clinical and Diagnostic Features
Acute-onset postoperative endophthalmitis after cataract surgery typically presents with pain, decreased vision, redness, and intraocular inflammation, often including fibrin and/or hypopyon (Figure 1).1 The traditional method of making a microbiologic diagnosis of endophthalmitis involves a vitreous aspirate followed by various special stains and cultures. Clinical research has also reported a potential role for polymerase chain reaction (PCR) testing and whole genome sequencing as more sensitive means of identifying causative microbiologic agents in cases of suspected endophthalmitis.2,3
Figure 1. Typical signs of endophthalmitis include (A) hypopyon, (B) fibrin, (C) anterior vitreous cell, and (D) prominent vitreous opacities and membrane formation (arrow) on B-scan ultrasonography. Images courtesy Harry W. Flynn Jr., MD.
Current reported rates of endophthalmitis following cataract surgery vary widely but generally range from about 0.02% to 0.2%.4,5 A 2022 report from Bascom Palmer Eye Institute reported a rate of acute-onset postoperative endophthalmitis of 0.068% (22 cases in 32,505 cataract surgeries).6 The incidence of postoperative endophthalmitis has declined substantially using evidence-based practices that have evolved over the past century.7 Antisepsis was gradually introduced in eye surgery in the 1870s. In 1874, Johann Friedrich Horner reported that his “failure rate” of cataract surgery declined from 6.6% in 211 surgeries from 1867 to 1870 (without antisepsis) to 1.5% in 397 surgeries from 1870 to 1875 (with antisepsis).8
Improvements in surgical incisions also improved outcomes. In 1884, Julius Jacobson reported a “failure rate” of 10% with a semicircular corneal incision, but only about 4% with the improved von Graefe incision.8 Leopold reported a halving of rates of endophthalmitis following cataract surgery from about 2% in 1920 to about 1% in 1940, which he attributed to further improvements in aseptic technique.9 The development of povidone-iodine (PI) in the 1950s was another important milestone.10
The introduction of prophylactic topical and subconjunctival antibiotics in the 1940s further reduced endophthalmitis rates. Allen and Mangiaracine reported a substantial reduction from 1945 to 1960. Specifically, in 13 case series published prior to 1950, the average rate was 1.16%; in 10 case series published from 1945 to 1960, the average rate was 0.21%. In 1964, Allen and Mangiaracine reported a single-center incidence of 0.11% (22 cases in 20,000 surgeries) and concluded, “the observed reduction in the rate of infection over the past 2 decades may be attributed to the use of antibiotics topically in the eye before surgery.”11
The decline in endophthalmitis rates from 1950 to 1964 is very impressive, from about 1% to about 0.1%, or a 10-fold decline. However, the further decline from 1964 to today is less impressive, from about 0.1% to about 0.068%, or only about a 1.5-fold decline. This may seem surprising when one considers the many advances in cataract surgery over the past 60 years, including phacoemulsification, smaller incisions, and foldable intraocular lenses (IOLs). This illustrates the important point that endophthalmitis cannot be prevented, and is in fact not a “never event.”12
Many investigators have studied the use of prophylactic antibiotics, and this practice is now common in many parts of the world. In 2007, the European Society of Cataract and Refractive Surgeons (ESCRS) published data from a randomized clinical trial evaluating the use of prophylactic intracameral cefuroxime administered at the time of cataract surgery. The pooled incidence rates of endophthalmitis in this study were about 0.07% in eyes receiving intracameral cefuroxime compared to about 0.35% in eyes not receiving intracameral cefuroxime, for about a 5-fold reduction.13 However, these results have been criticized and not universally adopted in clinical practice, particularly in many areas of the United States. The high rate of endophthalmitis without intracameral antibiotics (about 0.35%) may have exaggerated the apparent effect of the intracameral cefuroxime.7 In addition, the use of topical levofloxacin, rather than one of the more modern fourth-generation fluoroquinolones, also might have worsened the “background” rate of endophthalmitis and exaggerated the apparent effect of the intracameral cefuroxime.14 Nevertheless, in 2021, the American Society of Cataract and Refractive Surgeons (ASCRS) conducted a poll of its members and reported that about two-thirds of respondents regularly used intracameral antibiotics, predominantly (83%) off-label moxifloxacin. Of the respondents who did not use intracameral antibiotics, most indicated that they would use an affordable and approved formulation if it became available in the United States.15
Intravitreal injection use has increased exponentially since the introduction of intravitreal anti–vascular endothelial growth factor (VEGF) therapy for the treatment of macular diseases.16 At the time of their introduction, the administration of topical antibiotics after intravitreal injection was recommended for endophthalmitis prophylaxis. However, subsequent data have not demonstrated a benefit with topical antibiotics, and antibiotics are not typically used today.17 Furthermore, face-masking may not be necessary, although it is probably prudent, and a no-talking policy during injection is generally recommended to prevent contamination with oral flora.18 Other practices without clear consensus include the application of PI to the eyelids and the use of an eyelid speculum.
In 1945, Snell reported a 15.1% incidence of endophthalmitis after open globe injury (OGI).19 With time, rates of endophthalmitis after OGI have improved to around 4% in accordance with contemporary practices, including earlier wound closure and prompt initiation of systemic antibiotics.20 The standard route of systemic antibiotic administration varies by institution but in 2023, a meta-analysis involving 1,555 patients demonstrated noninferiority of oral vs intravenous antibiotic administration in the prevention of endophthalmitis after OGI.21 Organic intraocular foreign bodies (IOFBs) should be removed as soon as possible while nonorganic IOFBs may be removed later when the associated inflammation has decreased and clear media allows for better visualization and safer removal.22
Endogenous endophthalmitis was first reported by Haden in 1918 in a patient with meningococcal cerebrospinal meningitis; the patient was managed with intravenous antimeningococcal serum.23 Lewis and Wallace described another patient with endogenous endophthalmitis in 1946 who was managed with penicillin, sodium salicylate, and atropine sulfate ointment with resolution of the infection.24 In recent years, the incidence of endogenous endophthalmitis has increased with the corresponding increase in intravenous drug use in the United States, with a 4-fold increase in hospital admissions for endogenous endophthalmitis associated with drug use seen between 2003 to 2016.25 Although ophthalmologists were traditionally consulted for endophthalmitis screening in patients with Candida septicemia, the American Academy of Ophthalmology released a statement recommending against this practice in 2022, reserving consultation only for patients with signs or symptoms suggestive of ocular infection, or in neurologically impaired patients who cannot report a history of visual symptoms.26 Indeed, in 2023, Priluck and colleagues described a cohort of 81 eyes of 75 patients with fungal endophthalmitis, all of whom were symptomatic, further supporting the Academy’s screening guidelines.27
The recent identification of a novel fungal species, Candida auris, has developed into an international public health concern. Candida auris was first isolated in 2009 from the external ear canal of a 70-year-old patient from Japan.28 Since then, infections due to Candida auris have been reported in over 40 countries with mortality rates between 30% and 60% largely secondary to significant and sometimes untreatable drug resistance to all known antifungal classes.29 In 2022, Breazzano and colleagues described a case of endogenous panophthalmitis involving Candida auris in a 30-year-old immunocompromised male. The patient underwent enucleation and ultimately died despite treatment with intravitreal and systemic antifungals.30 Diagnostic methods employed by laboratories frequently misidentify Candida auris as other organisms, making diagnosis, management, and infection control efforts challenging.31
Treatment Strategies
Prior to the introduction of antibiotics, treatments for endophthalmitis included antiserum, mercury oxycyanide, topical mercurochrome, intravenous typhoid vaccine, intramuscular injection of boiled milk, and local x-rays.23,32 After the introduction of antibiotics in the early 1940s and until the early 1970s, standard treatment for endophthalmitis was hospitalization and intravenous antibiotics, with or without adjunctive topical, subconjunctival, and intracameral antibiotics.33 For example, in 1949, Givner reported a case of acute-onset postoperative Neisseria catarrhalis endophthalmitis treated by irrigating the anterior chamber with penicillin, placing penicillin-soaked pledgets in the conjunctival cul-de-sac, and systemic penicillin and sulfadiazine; visual acuity (VA) recovered to 20/20.34
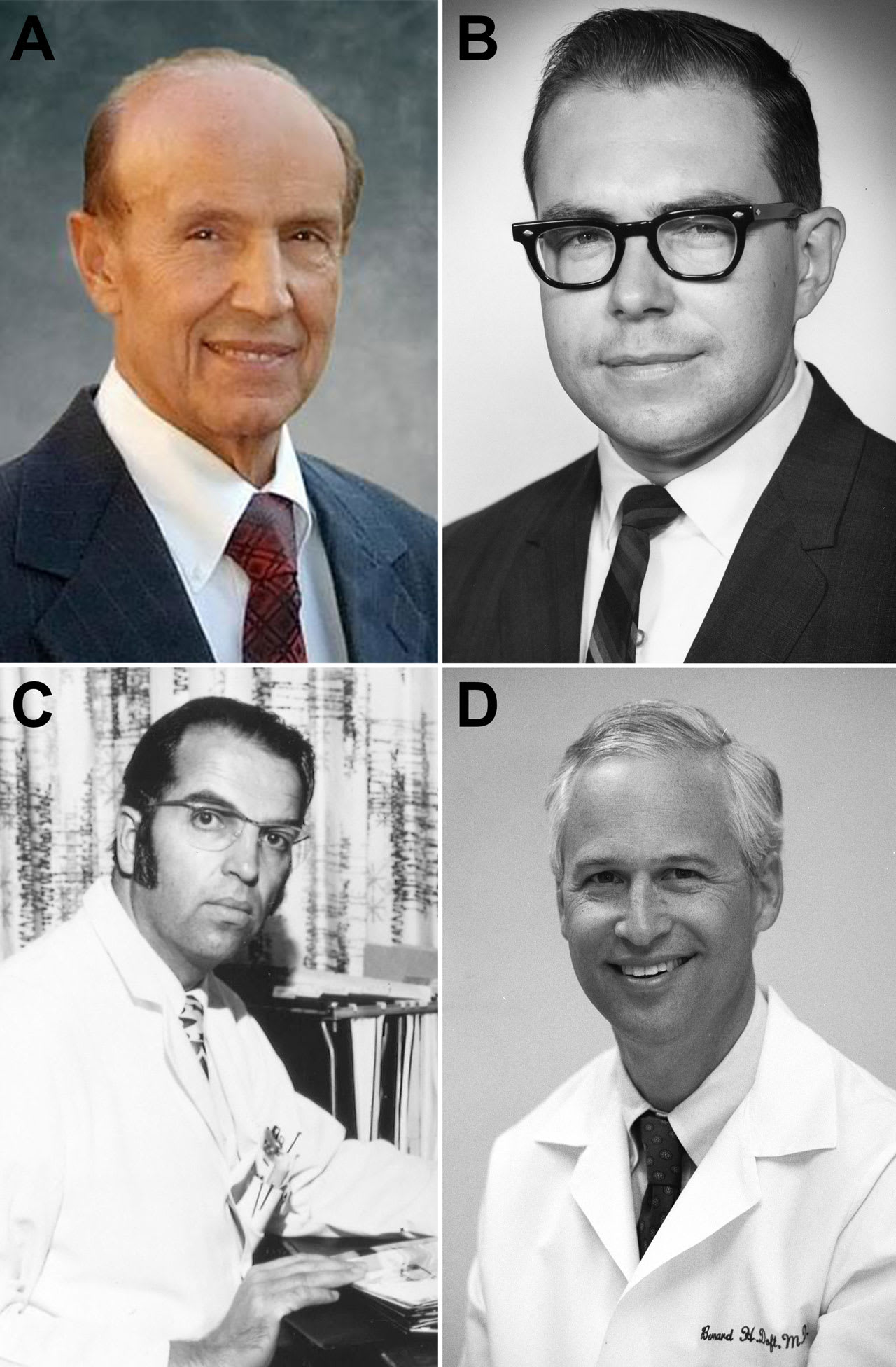
Figure 2. Key historical figures in endophthalmitis diagnosis and treatment. (A) Gholam Peyman, MD, developed techniques for intravitreal antimicrobial therapy; (B) Richard Forster, MD, studied clinical outcomes of intravitreal antimicrobial therapy; (C) Robert Machemer, MD, revolutionized endophthalmitis treatment by developing pars plana vitrectomy; (D) Bernard Doft, MD, was the principal investigator in the Endophthalmitis Vitrectomy Study. Images courtesy Harry W. Flynn Jr., MD.
In 1971, Leopold reviewed the increasing number of available antimicrobials for ophthalmologic use. At the time, agents were delivered systemically in high doses in an attempt to achieve therapeutic intraocular levels. Nevertheless, treatment outcomes were generally poor. The ineffectiveness of systemic and topical/subconjunctival antibiotics in the treatment of endophthalmitis led to the investigation of intravitreal antibiotic delivery by Peyman (Figure 2A) and colleagues using rabbit models in the early 1970s.35 Successful treatment of patients with intravitreal antimicrobials were reported soon after by Forster (Figure 2B) and others.36,37
Around the same time, Machemer (Figure 2C) and associates introduced pars plana vitrectomy (PPV) for the treatment of various vitreoretinal diseases.38 Machemer’s original instrument was the vitreous infusion suction cutter (VISC), although the instrumentation improved substantially over time. The advantages of PPV in the treatment of endophthalmitis were thought to include source control by debulking the infection, clearing of the visual axis to allow for visual rehabilitation and serial funduscopic examination, collection of adequate vitreous specimens for culture to guide management, and better distribution of intravitreal antibiotics in the vitrectomized eye.33
Intravenous antibiotics with or without intravitreal antibiotics were standard treatment for endophthalmitis in the 1970s, often requiring inpatient admission for 5 days or more. In 1987, Pavan and Brinser reported a series of 16 eyes treated with intravitreal and subconjunctival antibiotics, but no systemic antibiotics, with relatively good outcomes.39 Despite evidence suggesting improved outcomes with intravitreal antibiotics, most case series included patients with complex conditions and ocular comorbidities, making it difficult to differentiate the effect of systemic antibiotics and PPV on final visual results. To address these questions in the management of postoperative endophthalmitis, the Endophthalmitis Vitrectomy Study (EVS) was conducted in the late 1980s and early 1990s.
The EVS study group was organized under the leadership of Doft (Figure 2D) and the National Eye Institute to evaluate the roles of PPV and systemic antibiotics in the management of acute-onset endophthalmitis following cataract surgery or secondary IOL implantation. The outcomes of the EVS were reported at the 1995 annual meeting of the American Academy of Ophthalmology (AAO) and subsequently published in a series of articles. When initial VA was hand motions (HM) or better, there was no significant difference in VA outcomes between patients randomized to TAP or PPV. However, when initial VA was light perception (LP), PPV was associated with significantly more favorable VA outcomes. There was no difference in final VA or media clarity with or without intravenous antibiotics.40
In general, with some relatively minor exceptions, the guidelines of the EVS continue to be followed.33 Perhaps the most important change is the reduced usage of intravitreal amikacin, which, like other aminoglycosides (including gentamicin), can be associated with macular toxicity.41 Currently, ceftazidime or a similar third-generation cephalosporin is used instead.42 Another deviation from the original EVS protocol involves the use of systemic antibiotics. Although rarely used in the United States, systemic antibiotics are frequently administered today in Europe and in other parts of the world.15,43 In the United States, systemic antibiotics are frequently used in the treatment of patients with endogenous endophthalmitis or at times in endophthalmitis associated with severe ocular trauma and open globe injuries in some contexts.
In addition, PPV and cataract surgery were performed differently in 1995 than they are today. At that time, PPV used 20-gauge transscleral instrumentation, which may have had a higher risk of complications. Moreover, cataract surgery in 1995 consisted predominantly of extracapsular cataract extraction and scleral tunnel phacoemulsification, although additional studies have demonstrated similar findings with clear corneal incision phacoemulsification.7,44,45 Given the improvements in PPV instrumentation and techniques, some have suggested that indications for PPV in the treatment of endophthalmitis could be expanded, such as in patients with presenting VA of HM or better.
The EVS has continued to influence management to this day. Today, patients are generally managed without intravenous antibiotics and associated inpatient hospitalization. Rather, most patients are treated as outpatients in an office setting with vitreous tap and intravitreal antibiotic injection. This reduces both financial cost and treatment burden to the patient while not sacrificing outcomes. The economic implications of the EVS have been reported at an estimated annual savings of $7.6 to $40 million.46
Treatment regimens have also evolved. First-line intravitreal therapy is now generally vancomycin and ceftazidime (or a comparable third-generation cephalosporin). Subconjunctival agents are no longer routinely used except in select cases (eg, wound infection), because of post-EVS studies that reported no additional benefit.47,48
Some aspects of endophthalmitis management remain controversial. The use of steroids in acute-onset postoperative endophthalmitis is frequently debated.49 Although patients are no longer routinely prescribed oral prednisone due to systemic side effects, many clinicians have a low threshold for injecting dexamethasone intravitreally. A 2017 Cochrane Review concluded that, although some studies may show a benefit of adjunctive intravitreal steroid use, it is not possible to make a definitive conclusion regarding effectiveness given the paucity of studies and variable results.49
As smaller gauge instrumentation and improved viewing systems have been developed, the role of PPV has also changed. Some series have demonstrated good VA outcomes in patients with early PPV, particularly in patients with severe disease and those not responding to intravitreal antibiotics.50,51 Consequently, some retinal surgeons prefer early intervention with PPV.52 In cases of concurrent retinal detachment with endophthalmitis, silicone oil can also be considered.53
Conclusions
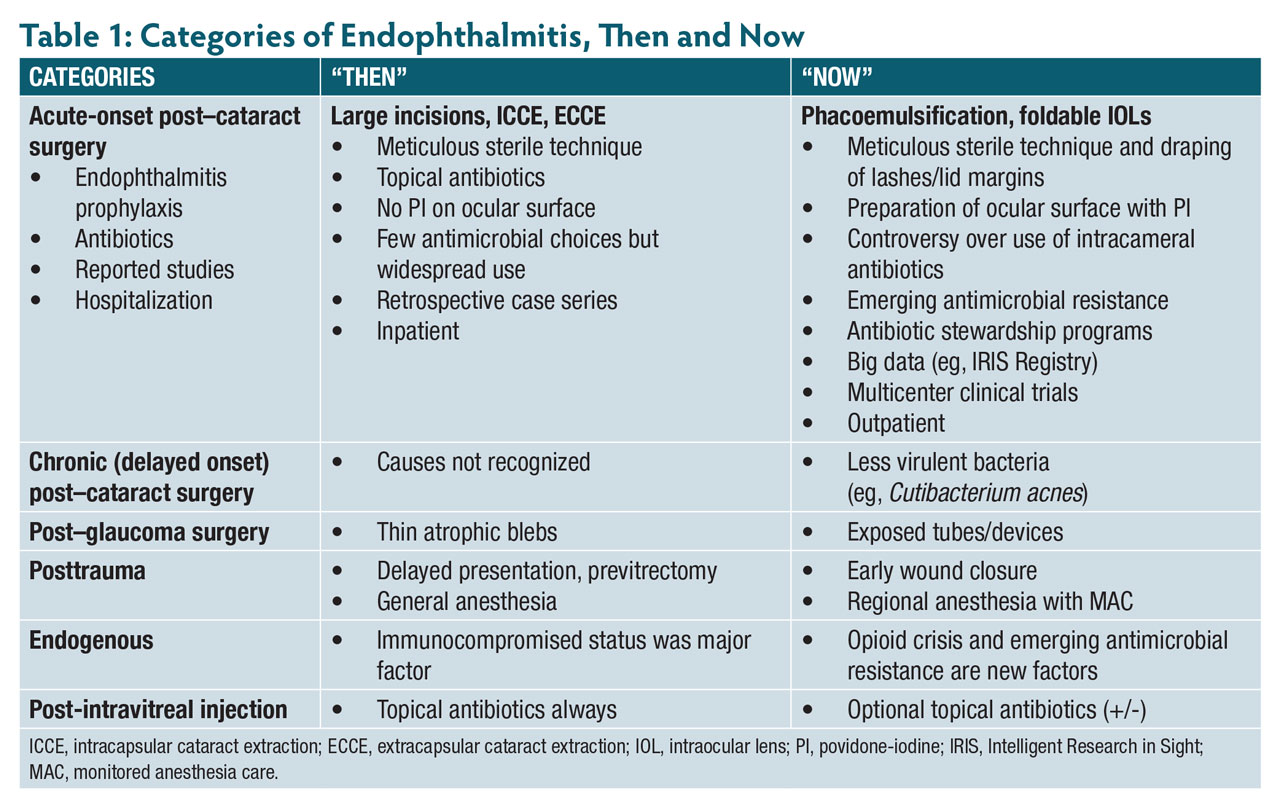
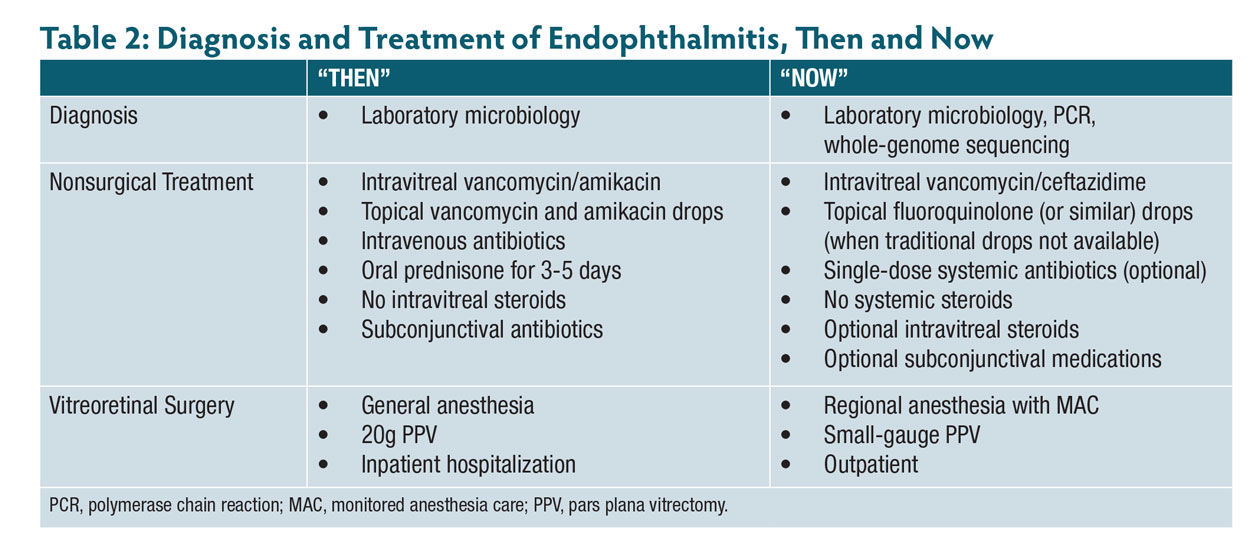
The incidence and management of endophthalmitis have evolved over time. Rates of endophthalmitis have decreased with the implementation of improved surgical techniques, antiseptic practices, and prophylactic antibiotics. The treatment of endophthalmitis (Table 1 and Table 2) has changed from using systemic intravenous antibiotics with prolonged inpatient stays to intravitreal antibiotics with or without oral antibiotics in the outpatient setting.54 Although intravitreal vancomycin remains a component of current first line-treatment, intravitreal amikacin has been replaced with ceftazidime due to reports of retinal toxicity. Intravitreal steroids, although not used in the EVS, are now occasionally used when a bacterial etiology is suspected. Surgical intervention, when indicated, has advanced from 20-gauge PPV under general anesthesia to small-gauge PPV with or without silicone oil tamponade under regional anesthesia with MAC. Potential future directions in the prevention, diagnosis, and management of endophthalmitis include the use of prophylactic intracameral antibiotics, advanced diagnostic techniques, and small-gauge PPV. By understanding the history and future directions of endophthalmitis, retina specialists will be better equipped to manage this often challenging condition. RP





References
1. Microbiologic factors and visual outcome in the endophthalmitis vitrectomy study. Am J Ophthalmol. 1996;122(6):830-846.
2. Sandhu HS, Hajrasouliha A, Kaplan HJ, Wang W. Diagnostic utility of quantitative polymerase chain reaction versus culture in endophthalmitis and uveitis. Ocul Immunol Inflamm. 2019;27(4):578-582.
3. Patel NA, Miller D, Relhan N, Alfonso EC, Flynn HW, Jr. Novel use of fluorescence in situ hybridization for the rapid identification of microorganisms in endophthalmitis and keratitis. Ophthalmic Surg Lasers Imaging Retina. 2019;50(5):S9-S12.
4. Sengillo JD, Chen Y, Perez Garcia D, Schwartz SG, Grzybowski A, Flynn HW, Jr. Postoperative endophthalmitis and toxic anterior segment syndrome prophylaxis: 2020 update. Ann Transl Med. 2020;8(22):1548.
5. Pershing S, Lum F, Hsu S, et al. Endophthalmitis after cataract surgery in the United States: a report from the Intelligent Research in Sight Registry, 2013-2017. Ophthalmology. 2020;127(2):151-158.
6. Kunkler AL, Sengillo JD, Al-Khersan H, et al. Acute-onset postoperative endophthalmitis after cataract surgery performed by resident and attending physicians at a university teaching hospital. J Cataract Refract Surg. 2022;48(11):1312-1317. doi:10.1097/j.jcrs.0000000000000989
7. Zafar S, Dun C, Srikumaran D, et al. Endophthalmitis rates among Medicare beneficiaries undergoing cataract surgery between 2011 and 2019. Ophthalmology. 2022;129(3):250-257.
8. Leffler C, Bansal S. The history of glaucoma. Amsterdam: Wayenborgh Publications; 2020.
9. Leopold IH. Management of intra-ocular infection. Trans Ophthalmol Soc U K (1962). 1971;91:577-610.
10. Shelanski HA, Shelanski MV. PVP-iodine: history, toxicity and therapeutic uses. J Int Coll Surg. 1956;25(6):727-734.
11. Allen HF, Mangiaracine AB. Bacterial endophthalmitis after cataract extraction. a study of 22 infections in 20,000 operations. Arch Ophthalmol. 1964;72:454-462.
12. Schachat AP, Rosenfeld PJ, Liesegang TJ, Stewart MW. Endophthalmitis is not a “never event.” Ophthalmology. 2012;119(8):1507-1508.
13. Barry P, Seal DV, Gettinby G, et al. ESCRS study of prophylaxis of postoperative endophthalmitis after cataract surgery: preliminary report of principal results from a European multicenter study. J Cataract Refract Surg. 2006;32(3):407-410.
14. O’Brien TP, Arshinoff SA, Mah FS. Perspectives on antibiotics for postoperative endophthalmitis prophylaxis: potential role of moxifloxacin. J Cataract Refract Surg. 2007;33(10):1790-1800.
15. Chang DF, Rhee DJ. Antibiotic prophylaxis of postoperative endophthalmitis after cataract surgery: results of the 2021 ASCRS member survey. J Cataract Refract Surg. 2022;48(1):3-7.
16. Chopra R, Preston GC, Keenan TDL, et al. Intravitreal injections: past trends and future projections within a UK tertiary hospital. Eye (Lond). 2022;36(7):1373-1378.
17. Baudin F, Benzenine E, Mariet AS, et al. Topical antibiotic prophylaxis and intravitreal injections: Impact on the incidence of acute endophthalmitis-A nationwide study in France from 2009 to 2018. Pharmaceutics. 2022;14(10).
18. Reyes-Capo DP, Yannuzzi NA, Smiddy WE, Flynn HW, Jr., Endophthalmitis/Anti-VEGF Study Group. Trends in endophthalmitis associated with intravitreal injection of anti-VEGF agents at a tertiary referral center. Ophthalmic Surg Lasers Imaging Retina. 2021;52(6):319-326.
19. Snell AC. Perforating ocular injuries. Am J Ophthalmol. 1945;28(3):263-281.
20. Hudson JL, Fan JC, Smiddy WE, Sridhar J, Yannuzzi NA, Flynn HW, Jr. Acute- and delayed-onset endophthalmitis after open globe injuries: clinical features and visual acuity outcomes. Retina. 2023;43(4):594-599.
21. Patterson TJ, McKinney D, Ritson J, et al. The use of preoperative prophylactic systemic antibiotics for the prevention of endopthalmitis in open globe injuries: A meta-analysis. Ophthalmol Retina. 2023;7(11):972-981.
22. Banker TP, McClellan AJ, Wilson BD, et al. Culture-positive endophthalmitis after open globe injuries with and without retained intraocular foreign bodies. Ophthalmic Surg Lasers Imaging Retina. 2017;48(8):632-637.
23. Haden H. Metastatic endophthalmitis associated by epidemic cerebro-spinal meninigitis. Am J Ophthalmology. 1918;1(9).
24. Lewis PM, Wallace GM. Metastatic endophthalmitis. Am J Ophthalmol. 1947;30(3):332.
25. Mir TA, Papudesu C, Fang W, Hinkle DM. Incidence of drug use-related endogenous endophthalmitis hospitalizations in the United States, 2003 to 2016. JAMA Ophthalmol. 2021;139(1):18-26.
26. Breazzano MP, Bond JB, 3rd, Bearelly S, et al. American Academy of Ophthalmology recommendations on screening for endogenous Candida endophthalmitis. Ophthalmology. 2022;129(1):73-76.
27. Priluck AZ, Huang P, Breazzano MP. Outcomes and clinical features predictive of fungal endophthalmitis. Am J Ophthalmol. 2023;251:104-114.
28. Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53(1):41-44.
29. Chowdhary A, Jain K, Chauhan N. Candida auris genetics and emergence. Annu Rev Microbiol. 2023;77:583-602.
30. Breazzano MP, Tooley AA, Godfrey KJ, Iacob CE, Yannuzzi NA, Flynn HW. Candida auris and endogenous panophthalmitis: clinical and histopathological features. Am J Ophthalmol Case Rep. 2020;19:100738.
31. Vila T, Sultan AS, Montelongo-Jauregui D, Jabra-Rizk MA. Candida auris: a fungus with identity crisis. Pathog Dis. 2020;78(4).
32. Sugar HS, Zekman T. Late infection of filtering conjunctival scars. Am J Ophthalmol. 1958;46(2):155-170.
33. Flynn HW Jr, Scott IU. Legacy of the Endophthalmitis Vitrectomy Study. Arch Ophthalmol. 2008;126(4):559-561. doi:10.1001/archopht.126.4.559
34. Givner I. Neisseria catarrhalis endophthalmitis; report of a case with complete recovery. Am J Ophthalmol. 1949;32(5):699.
35. Daily MJ, Peyman GA, Fishman G. Intravitreal injection of methicillin for treatment of endophthalmitis. Am J Ophthalmol. 1973;76(3):343-350. doi:10.1016/0002-9394(73)90489-3
36. Peyman GA, Herbst R. Bacterial endophthalmitis. treatment with intraocular injection of gentamicin and dexamethasone. Arch Ophthalmol. 1974;91(5):416-418. doi:10.1001/archopht.1974.03900060428017
37. Forster RK. Endophthalmitis. diagnostic cultures and visual results. Arch Ophthalmol. 1974;92(5):387-392. doi:10.1001/archopht.1974.01010010399005
38. Machemer R, Buettner H, Norton EW, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(4):813-820.
39. Pavan PR, Brinser JH. Exogenous bacterial endophthalmitis treated without systemic antibiotics. Am J Ophthalmol. 1987;104(2):121-126. doi:10.1016/0002-9394(87)90002-x
40. Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study. a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113(12):1479-1496.
41. Campochiaro PA, Lim JI, The Aminoglycoside Toxicity Study Group. Aminoglycoside toxicity in the treatment of endophthalmitis. Arch Ophthalmol. 1994;112(1):48-53. doi:10.1001/archopht.1994.01090130058017
42. Flynn HW, Relhan N, Schwartz SG, Iyer G, Lytvynchuk L, Grzybowski A. Endophthalmitis in Clinical Practice. 2nd ed. Switzerland: Springer Cham; 2023.
43. Grzybowski A, Turczynowska M, Schwartz SG, Relhan N, Flynn HW, Jr. The role of systemic antimicrobials in the treatment of endophthalmitis: a review and an international perspective. Ophthalmol Ther. 2020;9(3):485-498. doi:10.1007/s40123-020-00270-w
44. Yannuzzi NA, Si N, Relhan N, et al. Endophthalmitis after clear corneal cataract surgery: outcomes over two decades. Am J Ophthalmol. 2017;174:155-159. doi:10.1016/j.ajo.2016.11.006
45. Rahmani S, Eliott D. Postoperative endophthalmitis: a review of risk factors, prophylaxis, incidence, microbiology, treatment, and outcomes. Semin Ophthalmol. 2018;33(1):95-101. doi:10.1080/08820538.2017.1353826
46. Wisniewski SR, Hammer ME, Grizzard WS, et al. An investigation of the hospital charges related to the treatment of endophthalmitis in the Endophthalmitis Vitrectomy Study. Ophthalmology. 1997;104(5):739-745. doi:10.1016/s0161-6420(97)30239-5
47. Smiddy WE, Smiddy RJ, Ba’Arath B, et al. Subconjunctival antibiotics in the treatment of endophthalmitis managed without vitrectomy. Retina. 2005;25(6):751-758. doi:10.1097/00006982-200509000-00011
48. Iyer MN, Han DP, Yun HJ, et al. Subconjunctival antibiotics for acute postcataract extraction endophthalmitis—is it necessary? Am J Ophthalmol. 2004;137(6):1120-1121. doi:10.1016/j.ajo.2003.12.042
49. Kim CH, Chen MF, Coleman AL. Adjunctive steroid therapy versus antibiotics alone for acute endophthalmitis after intraocular procedure. Cochrane Database Syst Rev. 2017;2(2):CD012131. doi:10.1002/14651858.CD012131.pub2
50. Panahi P, Mirzakouchaki-Borujeni N, Pourdakan O, Arevalo JF. Early vitrectomy for endophthalmitis: are EVS guidelines still valid? Ophthalmic Res. 2023;66(1):1318-1326. doi:10.1159/000534650
51. Kuhn F, Gini G. Ten years after... are findings of the Endophthalmitis Vitrectomy Study still relevant today? Graefes Arch Clin Exp Ophthalmol. 2005;243(12):1197-1199. doi:10.1007/s00417-005-0082-8
52. Das T, Joseph J, Simunovic MP, et al. Consensus and controversies in the science of endophthalmitis management: basic research and clinical perspectives. Prog Retin Eye Res. 2023;97:101218. doi:10.1016/j.preteyeres.2023.101218
53. Sinisi F, Della Santina M, Loiudice P, Figus M, Casini G. The role of silicone oil in the surgical management of endophthalmitis: a systematic review. J Clin Med. 2022;11(18). doi:10.3390/jcm11185445
54. Rohowetz LJ, Yi JS, Gowaily K, et al. Open globe injuries with retained intraocular foreign bodies: anesthesia options and endophthalmitis rates. J Vitreoretin Dis. In Press.