





Development of vitreoretinal surgery capacity in resource-limited settings is extremely challenging because of the substantial resource requirements and subspecialty training involved.1 During a mission to Freetown, Sierra Leone, in March 2026, our surgical team confronted a sobering reality: The cost of supplies for a single complex retinal detachment repair could fund hundreds of cataract surgeries. In a region with a significant shortage of primary ophthalmic care, the question naturally arises whether a retina-focused mission represents the most effective use of limited resources.
The Ebola outbreak of 2014-2016 provided the impetus for establishing infrastructure capable of supporting the most advanced vitreoretinal surgical capacity in West Africa outside of Ghana and Morocco (Figure 1). Central Global Vision Fund, a Christian nonprofit organization supporting eye care needs in Sierra Leone and other underserved regions worldwide, and Connaught Hospital in Freetown, the country’s largest government hospital, supported the initiative. That collaboration between Steven Yeh, MD, professor and Stanley Truhlsen Jr. Chair of the Truhlsen Eye Institute at the University of Nebraska Medical Center in Omaha, and local ophthalmologist Lloyd Harrison-Williams, MBBS, began in 2015 (Figure 2). Their initial efforts focused on ophthalmic complications in Ebola survivors, as well as evaluation of close contacts from the outbreak. These efforts ultimately led to development of the Ebola Virus Persistence in Ocular Tissues and Fluids (EVICT) study, which aimed to determine whether Ebola virus persisted in immune-privileged sites such as the eye.2-4 Determining whether Ebola virus could persist in the vitreous was particularly important, and vitreoretinal surgical infrastructure was needed to evaluate vitreous samples from Ebola survivors, close contacts, and controls, including patients with retinal detachment and other surgical indications.

Figure 1. Map of West Africa with the outline of the United States overlaid for scale. Freetown, Sierra Leone, is marked with a star. The nearest centers with vitreoretinal surgical capacity are in Agadir, Morocco, and Kumasi, Ghana.
In 2023, Grant A. Justin, MD, of the Walter Reed National Military Medical Center in Bethesda, Maryland, joined Drs. Harrison-Williams and Yeh to perform the first vitrectomies in

Figure 2. Steven Yeh, MD, and Lloyd Harrison-Williams, MBBS, at Connaught General Hospital in Freetown, Sierra Leone. Their collaboration began in 2015 during the West African Ebola outbreak.
Sierra Leone. By March 2026, approximately 400 cases had been performed. Furthermore, Lloyd B. Williams, MD, PhD, of Duke Eye Center in Durham, North Carolina, has performed approximately 100 corneal transplants in Sierra Leone since 2021, demonstrating that complex ophthalmic care can be delivered in resource-limited settings.
Although these initial efforts represent only a small fraction of the tremendous regional need, the broader objective has been the development of sustainable subspecialty care. Through collaboration with and training of Sierra Leonian ophthalmic surgeons, the team sought to leave behind more than successful surgical outcomes—the goal was to establish the foundation for a lasting West African vitreoretinal surgery program (Figure 3).

Figure 3. Lloyd Harrison-Williams, MBBS, performs vitreoretinal surgery at Lowell and Ruth Gess United Methodist Eye Hospital in Freetown. Established in 1984, the hospital is the largest and best equipped eye care facility in Sierra Leone and provides cataract care for patients from Sierra Leone as well as neighboring Guinea and Liberia.
The Logistical Landscape
Freetown is a city of striking contrasts, where modern surgical ambition intersects with fragile infrastructure. The city’s electrical power is supplied by a Turkish ship anchored in the harbor, necessitating surge protectors, backup generators, and constant vigilance regarding power supply stability during surgery. Sierra Leone has also been devastated by 2 major disasters over the past 35 years: a decade-long civil war during the 1990s, still visible in buildings marked by rocket-propelled grenade damage (Figure 4), and the Ebola outbreaks of the 2010s.
Logistics remain the primary challenge. Supply chains are frequently disrupted by significant delays in shipping and customs clearance. At times, the surgical team faced the possibility of running out of essential gases such as compressed nitrogen, prompting the use of compressed air to operate vitrectomy equipment.

Figure 4. Damage from Sierra Leone’s civil war (1991-2002) remains visible throughout Freetown, including this building near Connaught General Hospital that was damaged by a rocket-propelled grenade.
Environmental factors also posed a persistent threat to vitreoretinal equipment. Humid coastal air and periodic electrical outages with elevated room temperatures increased the risk of corrosion within surgical machinery, necessitating portable dehumidifiers and environmental temperature control. Most surgical vitrectomy equipment had to be imported because of limited local resources. To make these missions sustainable, there remains a pressing need for more affordable systems, stronger international supply partnerships, and development of revenue streams capable of supporting complex eye care in lower-middle-income countries.
Vitrectomy: Innovation Under Pressure
In a standard US operating room, ergonomics and equipment are often taken for granted. In Sierra Leone, many problems required ingenuity from the local staff. To prevent patients from inhaling the surgical drape, nurses suggested repurposing COVID-19 face shields as spacers, allowing patients to breathe comfortably under the drape while maintaining a sterile field.
The initial operating table was wood; the legs had to be cut to achieve a workable height. Even then, the table lacked adjustable headrests typical of ophthalmic surgical beds, complicating surgical positioning and stabilization.

Figure 5. Hand-welded dovetail attachment used to adapt the BIOM viewing system to an anterior-segment microscope, secured with tape for support.
Visualization remained a constant challenge, with clear views often lasting only an hour because of environmental factors, corneal edema, and equipment limitations. The team ultimately hired a local welder to fabricate a dovetail attachment that allowed a BIOM viewing system to be mounted onto an anterior-segment microscope to achieve adequate posterior-segment visualization (Figure 5).
Resource scarcity dictated many clinical decisions. Traditional gas tamponades are unavailable, so our team was forced to rely on silicone oil or air. The team adapted whenever possible, including the use of Lactated Ringer solution for infusion fluid and manual injection of silicone oil when automated systems were unavailable (Figure 6).

Figure 6. Manual injection of silicone oil tamponade during vitreoretinal surgery in Sierra Leone.
The surgical cases were often advanced and highly complex. The team suspected a possible collagen abnormality, such as Stickler syndrome, because many patients presented with atypical fibrous vitreous and giant retinal tears (Figure 7). Most patients with retinal detachment were not myopic and had shorter axial lengths with different anatomy, requiring placement of cannulas 0.5 mm closer to the limbus.
In addition, limited access to anti-VEGF therapy and the lack of lasers for panretinal photocoagulation (PRP) complicated management of proliferative diabetic retinopathy and sickle cell retinopathy, frequently resulting in vitreous hemorrhage requiring surgical intervention. The team now travels with a portable indirect laser for PRP during mission trips (Figure 8).
Beyond surgical mentorship, the program recognized that long-term success depends on training a skilled local support staff. Vitreoretinal surgery requires specialized sterile technique and meticulous handling of delicate instruments. Dr. Yeh has implemented dedicated protocols for each step of surgical turnover, standardizing workflows from retrobulbar block administration through patching, shielding, sterilization, and preparation for subsequent procedures.
Lensectomy and Scleral Buckling: Adapting to Resource Constraints
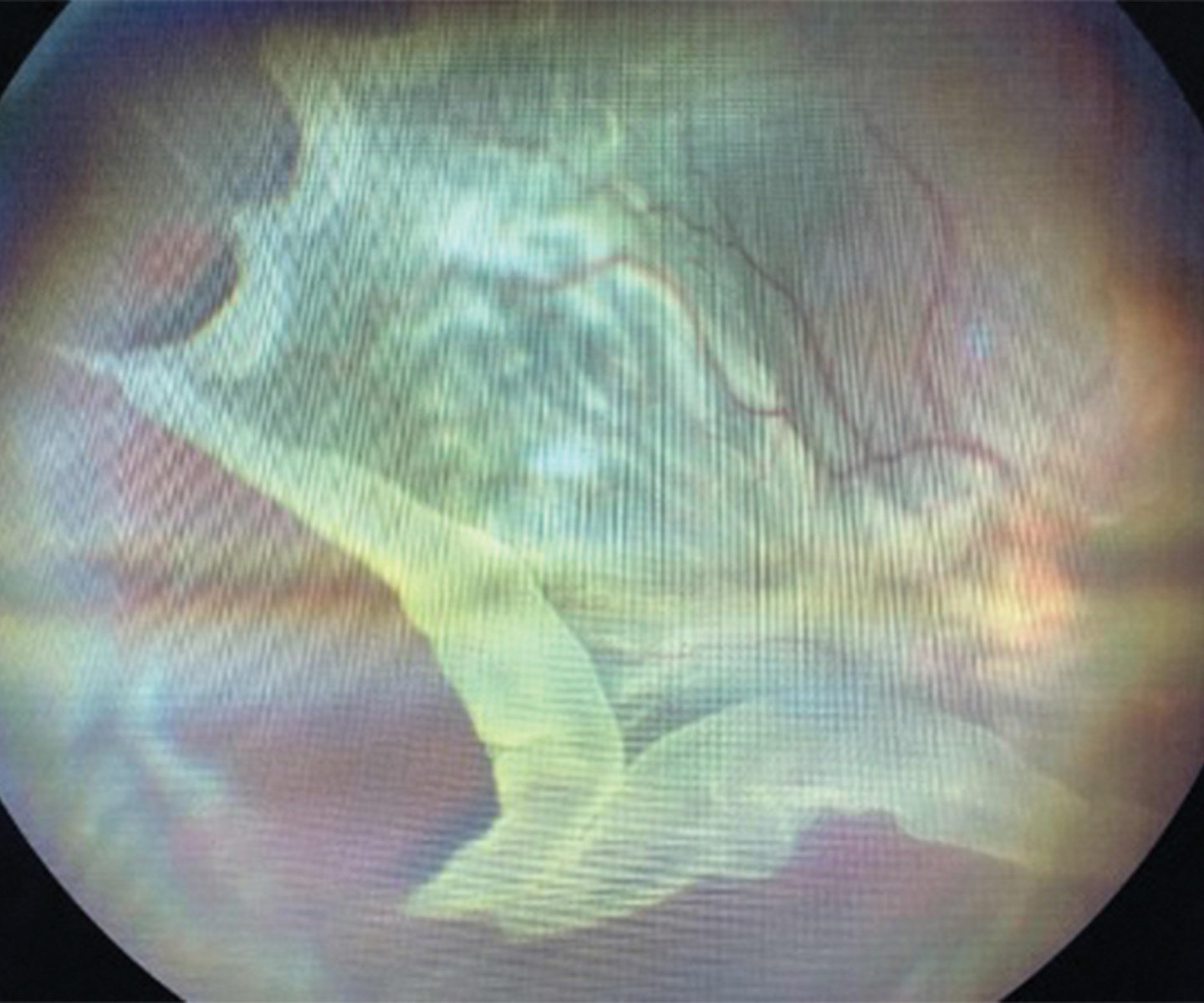
Figure 7 (Right). Fundus photograph demonstrating a chronic retinal detachment associated with a giant retinal tear.
Phacoemulsification capacity in Sierra Leone is extremely limited. As in many regions without access to phacoemulsification, ophthalmologists and surgical nurses frequently perform manual small-incision cataract surgery (MSICS). Because silicone oil is often required for retinal detachment repair, the team attempts to arrange MSICS before vitrectomy whenever possible.
Management of uveitic cases frequently necessitates pars plana lensectomy, although lensectomy is avoided whenever possible to minimize postoperative inflammation and refractive error in a setting where access to optical shops is limited. In addition, the absence of straight fragmatome needles required adaptation through use of curved phacoemulsification needles for posterior-segment work. West Africa needs its own Aurolab, like the low-cost ophthalmic manufacturing facility affiliated with the Aravind Eye Hospital in India, which could employ local men and women to manufacture sutures, lenses, and other ophthalmic supplies at lower cost.
Scleral buckling is particularly difficult in Sierra Leone, even with regional anesthesia, because of limited anesthesiology support for cardiac monitoring and pain management. Only 1 pediatric patient underwent scleral buckle surgery in 2025, representing the first such procedure in Sierra Leone in more than 30 years. The retina remained fully attached at postoperative year 1. Nevertheless, although the surgery was successful, scleral buckle surgery and the risk of cardiac complications must be carefully considered.
Conclusion: Cultivating a Sustainable Future

Figure 8 (Left). Lloyd Harrison-Williams, MBBS, performs panretinal photocoagulation for proliferative diabetic retinopathy using a portable indirect laser system.
For vitreoretinal surgery to become truly sustainable in West Africa, systemic change will be essential. Successful training of local surgeons such as Dr. Lloyd Harrison-Williams creates a lasting regional impact that far exceeds the immediate surgical volume. Demonstrating advanced surgical capabilities to the Sierra Leonean government also represents an important step toward validating the country’s National Eye Care Programme and advocating for improved long-term domestic funding for eye care.
Building this foundation will require changes in both logistics and workforce development. The team identified a need to transition to a single 23-gauge vitrectomy platform to simplify supply chains and has begun sourcing supplies from manufacturers in India to reduce costs. Equally important is the specialized training of local scrub technicians and nurses in sterile technique and instrument handling, along with protocolization of all aspects of surgical turnover. Because high-quality visualization remains central to successful vitreoretinal surgery, investment in advanced surgical microscopes is truly “worth its weight in gold.”
Ultimately, Dr. Yeh’s and Dr. Harrison-Williams’ vitreoretinal surgery program reflects both the resilience of the local medical community and the importance of subspecialty training in lower-middle-income countries. Our time in Freetown, Sierra Leone, has resulted in lifelong friendships and a renewed commitment to global health. We look forward to returning to continue our work with the Central Global Vision Fund to provide the essential supplies and equipment—from ophthalmic beds to surgical microscopes—required to make advanced retina care a lasting reality in Sierra Leone. RP





References
1. Retinal diseases and VISION 2020. Community Eye Health. 2003;16(46):19-20.
2. Yeh S, Shantha JG, Hayek B, Crozier I, Smith JR. Clinical manifestations and pathogenesis of uveitis in Ebola virus disease survivors. Ocul Immunol Inflamm. 2018;26(7):1128-1134. doi:10.1080/09273948.2018.1484493
3. Berry DE, Bavinger JC, Fernandes A, et al. Posterior segment ophthalmic manifestations in Ebola survivors, Sierra Leone. Ophthalmology. 2021;128(9):1371-1373. doi:10.1016/j.ophtha.2021.02.001
4. Hartley CD, Linderman S, Fashina T, et al. Understanding the pathogenesis of uveitis in Ebola virus disease survivors: an observational cohort and cross-sectional study protocol for clinical, molecular virologic and immunologic characterisation. BMJ Open. 2025;15(12):e104843. doi:10.1136/bmjopen-2025-104843